Abdominal pain
Common causes of abdominal pain :
Abdominal wall pain
Pain arising from the abdominal wall is usually constant and aching.
Movement, prolonged standing, and pressure accentuate the discomfort and muscle spasm.
This kind of pain may arise from a disease of the muscle (myositis, trauma and hematoma, muscle strain), nerve disease (diabetic neuropathy, postherpetic neuralgia), or it could be referred pain from an internal abdominal organ.
Abdominal wall pain often presents with a dermatomic pattern.
Characteristically, it starts off as sharp initially and can become dull over time. Coughing, sneezing, or lifting heavy weights may increase the pain, while applying heat or changing positions may relieve abdominal wall pain

Visceral pain
The best approach for visceral pain is according to location of pain and taking into account any associated symptoms to help guide the diagnosis.
Location is most easily categorized on the basis of embryologic origin. Pain located between the xiphoid process and the umbilicus originates in the foregut, which includes the distal esophagus, stomach, proximal duodenum, biliary tree, pancreas, and liver (although conditions of the liver usually do not cause chronic abdominal pain).
Pain in the periumbilical region arises from viscera of the midgut (eg, small intestine, appendix, ascending colon, proximal two thirds of the transverse colon).
Pain between the umbilicus and the symphysis pubis emanates from hindgut organs (eg, distal one third of the transverse colon, descending colon, rectosigmoid region).
1. The foregut

Pain in the epigastric area 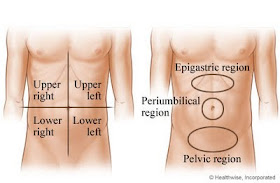
The epigastrium is an area of the central abdomen lying just below the sternum.
Common causes are dyspepsia, peritonitis, pancreatitis, GI obstruction, gall bladder disease and peptic ulcer and ruptured aortic aneurysm. Other causes include inflammatory bowel syndrome, gastric cancer, referred pain (from a myocardial infarction, pleural disease or spinal disease) and psychosomatic diseases.
Pain in the right upper quadrant (hypochondrium)
Causes of right upper quadrant pain include liver diseases, gall bladder disease, lesions of the hepatic flexure of the colon (carcinoma, diverticulosis, ischaemic colitis, Chron’s disease, atypical appendicitis or even constipation), renal diseases (pyelonephritis, nephro-lithiasis, hydronephrosis, renal carcinoma or other disease of the kidney or ureter, including obstruction of the urinary tract) or a dissecting aneurysm. Other causes include referred pain from the heart or a respiratory disease of the lower lobe of the lungs (lobar pneumonia or infarction from pulmonary embolism).
Many metabolic diseases can give the same picture including, diabetic ketoacidosis, Addisionian crisis, adrenal tuberculosis and metastatic carcinoma. Infections such as herpes zoster or a subphrenic abscess can also lead to pain in the right upper quadrant.
Pain in the left upper quadrant (hypochondrium)
Left upper quadrant pain is commonly associated with colonic diseases or splenic diseases. The spleen may be enlarged or may be the seat of an infarction. Diseases of the colon may include anything from distension of the splenic flexure of the colon as in cases of irritable bowel syndrome to colonic cancer.
2. The midgut
Pain in the periumbulical region
Causes of periumbulical pain include intestinal obstruction, mesenteric occlusion or enteritis.
3. The hindgut
Right lower quadrant pain
Pain in the right lower quadrant may be diffuse, as in early appendicitis, or crampy and nonradiating, as in ectopic pregnancy. Colon obstruction secondary to colon cancer, diverticulitis, and ureterolithiasis are common causes of pain in this area. Yersinia enterocolitica and Campylobacter sp., may mimic appendicitis and cause right lower quadrant pain, anorexia, low grade fever, and vomiting preceding the onset of diarrhea leading to a syndrome of mesenteric adenitis (lymph node enlargement) and terminal ileitis. The classic presentation of Crohn’s disease is that of colicky right lower quadrant pain and diarrhea. Low-grade fever and weight loss are frequently present as well. High fever indicates a possible infectious complication (ie, abscess). Hematochezia occurs in a minority of patients, most often in those with colonic involvement.
In women right lower quadrant pain could be a manifestation of pelvic inflammatory disease, acute salpingitis, ectopic pregnancy, ovarian cysts, abscesses and tumors in addition to the causes listed above. Cancer of the cecum, ileal carcinoid, lymphosarcoma, systemic vasculitis, radiation enteritis, ileocecal TB, and ameboma should be excluded.
Left lower quadrant pain
Diverticulitis, inflammatory bowel disease, pelvic inflammatory disease, a kidney stone, endometriosis, ectopic pregnancy, and rupture of an ovarian cyst are common causes of abdominal pain in this area.
Pain in the hypogastrium and pelvis
Common causes of pain in this area include rectal disease (rectal cancer, proctitis); bladder disease (stones, cystitis, bladder cancer) and more importantly in females (salpingo-oopheritis, uterine cancer).
Pain in the costovertebral angle
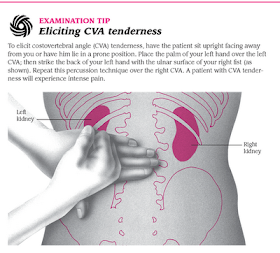
This is usually attributed to renal causes (kidney stones, pyelonephritis and malignancy).
Clinical features of abdominal pain
Intensity and description of pain
Dull, gnawing sensation of mild to moderate severity can be caused by peptic ulcer disease.
Extremely intense pain of sudden onset may be the result of mesenteric ischemia or perforated peptic ulcer.
Renal colic refers to episodic pain with intervening pain-free intervals.
Biliary pain typically presents with constant, steady pain without intervening pain-free intervals.
Severe intensity and a “tearing” quality can be caused by a dissecting aneurysms causes pain.
Patients with postprandial pain, food avoidance, weight loss, and known atherosclerotic disease should be evaluated for mesenteric angina.
Time course
Sudden onset (over seconds to minutes) of abdominal pain suggests a catastrophic event such as a ruptured abdominal aneurysm, ruptured ectopic pregnancy, or perforated peptic ulcer.
Rapidly progressive (over 1-2 hours) pain is seen typically in pancreatitis, cholecystitis, diverticulitis, bowel obstruction, renal or biliary colic, and mesenteric ischemia.
Gradual (over several hours) pain that progresses more slowly is more typical of peptic ulcer disease, distal small bowel obstruction, appendicitis, pyelonephritis, pelvic inflammatory disease, and malignant neoplasm, although it may be seen with many of the diagnoses in the more rapidly progressive categories as well.
Pain occurring following the onset of vomiting often indicates a medical illness, whereas pain that precedes vomiting often indicates a surgical illness. Persistence of pain for over 6 hours after acute onset has a high likelihood of a surgical cause and requires admission for observation.
Aggravating or alleviating factors
Pain relieved by antacids suggests peptic ulcer disease or esophagitis.
Pain worsened by movement suggests peritonitis, whereas constant movement by the patient in an attempt to find a comfortable position is commonly seen in bowel obstruction and renal colic.
Patients with partial relief by leaning forward, and aggravation by lying supine suggests a retroperitoneal process (such as pancreatitis) commonly find
Pain relieved by defecation may suggest a colonic source.
Patients with postprandial pain, food avoidance, weight loss, and known atherosclerotic disease should be evaluated for chronic intestinal ischemia (mesenteric angina) or intermittent intestinal obstruction (from internal or abdominal wall hernias, adhesions, or Crohn’s disease).
Pain that occurs at approximately monthly intervals should raise the suspicion of endometriosis or Mittelschmerz.
Physical examination
Vital signs
Tachycardia & hypotension: Vital signs may show tachycardia and hypotension indicative of intraabdominal hemorrhage or septic shock.
Fever: The fever of appendicitis, diverticulitis, and cholecystitis is typically low grade, whereas high fevers are seen in cases of cholangitis, urinary tract infections, pelvic inflammatory disease, or perforation of a viscus with frank peritonitis.
Inspection
Abdominal distention: Abdominal distention may suggest bowel obstruction or the presence of ascites.
Scaphoid abdomen: A scaphoid, tense abdomen is seen in cases of peritonitis.
Auscultation
Auscultation of the abdomen should be performed before palpation or percussion so as not to interfere with the interpretation of bowel sounds.
Absence of bowel sounds: Absence of bowel sounds is a sign of diffuse peritonitis.
Hyperactive bowel sounds: Intermittent hyperactive bowel sounds occurring concurrently with worsening of pain suggest a bowel obstruction. High-pitched hyperactive bowel sounds may also be seen in gastroenteritis.
Succussion splash: The presence of a succussion splash suggests gastric outlet obstruction.
Percussion
Tenderness on percussion: Percussion of the abdomen allows assessment of the presence of peritonitis. Pain produced by light tapping indicates inflammation of the parietal peritoneum. This pain may also be elicited by asking the patient to cough or by gently agitating the gurney upon which the patient is lying.
Tympany: A distended abdomen with tympany upon percussion suggests a bowel obstruction.
Palpation
Tightening (rigidity) of the abdominal wall musculature occurs as a reflexive response to peritoneal inflammation (voluntary guarding refers to tightness or rigidity of the abdomen that relaxes when the patient takes a deep breath, whereas involuntary guarding refers to rigidity of the abdominal wall musculature that does not relax in response to deep inspiration). Involuntary guarding indicates peritoneal inflammation.
Tenderness over McBurney’s point should be considered very strong evidence of appendicitis.
Cholecystitis and salpingitis are often well localized as well, and salpingitis may be confused with appendicitis.
Patients with an unimpressive abdominal examination and complaints of severe, worsening pain should be suspected of having mesenteric infarction.
Murphy’s sign refers to pain produced by deep inspiration during palpation of the right subcostal area and suggests acute cholecystitis.
Pain produced by lightly punching the costovertebral angle (”punch tenderness”) is often present in pyelonephritis.
Carnett’s test refers to the response of pain when the patient tenses the abdominal wall muscles by raising their head off the examination table. Worsening of pain during this maneuver suggests an abdominal wall source whereas improvement in the pain suggests a visceral origin.
The iliopsoas sign refers to pain produced by passive extension of the leg and suggests a psoas abscess.
The obturator sign refers to pain produced by rotation of the thigh in a flexed position.
A rectal examination can reveal focal tenderness from an intraabdominal abscess or appendicitis.
A pelvic examination is mandatory in female patients to look for evidence of salpingitis or adnexal masses.
The inguinal and femoral canals, umbilicus, and surgical scars should be evaluated for the presence of incarcerating hernias.
Once a cause is suspected the appropriate diagnostic procedure for the provisional diagnosis is selected.
Diagnosis
If the picture is obscure then the following important points and causes should be taken into account:
Ruptured ectopic pregnancy in females
Dissecting aortic aneurysm: Absence of tenderness and rigidity in the presence of continuous, diffuse pain in a patient likely to have vascular disease is quite characteristic of occlusion of the superior mesenteric artery. Abdominal pain with radiation to the sacral region, flank, or genitalia should always signal the possible presence of a rupturing abdominal aortic aneurysm. This pain may persist over a period of several days before rupture and collapse occur.
Peritoneal pain: Rigidity, rebound tenderness, fever and leucocytosis
Metabolic causes
Familial mediterranean fever
Diabetic ketoacidosis
Irritable bowel syndrome: Is the commonest cause of abdominal pain and should always be kept in mind.
If the cause of abdominal pain is still unclear, investigations that can be requested include:
Lab work
X-rays (supine, erect, lateral view)
Ultrasound
CAT scan
Laparoscopy
Operation vs. watchful waiting
Chronic abdominal pain
Chronic pain usually has persisted for 3 to 6 months and is affecting the patient’s activities of daily living. Often, the diagnosis can be made through history taking.
Chronic epigastric pain can be caused by peptic ulcer, chronic pancreatitis, GERD, dyspepsia, gall bladder disease.
Chronic lower abdominal pain can be caused by irritable bowel syndrome, inflammatory bowel disease, cancer. Right lower quadrant fullness and pain or perianal disease may indicate Crohn’s disease.
Less common causes include causes in the abdominal wall, fibromyalgia, hernia, referred pain, metabolic disorders (porphyria, chronic renal failure, and Addison’s disease) and psychological disorders.
The evaluation of chronic abdominal pain in a patient younger than 50 years old typically begins with ruling out the presence of alarm symptoms (weight loss, gastrointestinal bleeding, anemia, fever, or frequent nocturnal symptoms).
If no alarm symptoms are present and the patient has altered bowel habits then evaluation for irritable bowel syndrome is considered. This my include a CBC, TSH and electrolyte levels, and examination with flexible sigmoidoscopy.
Those with alarm symptoms or age above 50 years old may require a referral to a gastroenterologist.
Clinical features of abdominal pain
Intensity and description of pain
Dull, gnawing sensation of mild to moderate severity can be caused by peptic ulcer disease.
Extremely intense pain of sudden onset may be the result of mesenteric ischemia or perforated peptic ulcer.
Renal colic refers to episodic pain with intervening pain-free intervals.
Biliary pain typically presents with constant, steady pain without intervening pain-free intervals.
Severe intensity and a “tearing” quality can be caused by a dissecting aneurysms causes pain.
Patients with postprandial pain, food avoidance, weight loss, and known atherosclerotic disease should be evaluated for mesenteric angina.
Time course
Sudden onset (over seconds to minutes) of abdominal pain suggests a catastrophic event such as a ruptured abdominal aneurysm, ruptured ectopic pregnancy, or perforated peptic ulcer.
Rapidly progressive (over 1-2 hours) pain is seen typically in pancreatitis, cholecystitis, diverticulitis, bowel obstruction, renal or biliary colic, and mesenteric ischemia.
Gradual (over several hours) pain that progresses more slowly is more typical of peptic ulcer disease, distal small bowel obstruction, appendicitis, pyelonephritis, pelvic inflammatory disease, and malignant neoplasm, although it may be seen with many of the diagnoses in the more rapidly progressive categories as well.
Pain occurring following the onset of vomiting often indicates a medical illness, whereas pain that precedes vomiting often indicates a surgical illness. Persistence of pain for over 6 hours after acute onset has a high likelihood of a surgical cause and requires admission for observation.
Aggravating or alleviating factors
Pain relieved by antacids suggests peptic ulcer disease or esophagitis.
Pain worsened by movement suggests peritonitis, whereas constant movement by the patient in an attempt to find a comfortable position is commonly seen in bowel obstruction and renal colic.
Patients with partial relief by leaning forward, and aggravation by lying supine suggests a retroperitoneal process (such as pancreatitis) commonly find
Pain relieved by defecation may suggest a colonic source.
Patients with postprandial pain, food avoidance, weight loss, and known atherosclerotic disease should be evaluated for chronic intestinal ischemia (mesenteric angina) or intermittent intestinal obstruction (from internal or abdominal wall hernias, adhesions, or Crohn’s disease).
Pain that occurs at approximately monthly intervals should raise the suspicion of endometriosis or Mittelschmerz.
Physical examination
Vital signs
Tachycardia & hypotension: Vital signs may show tachycardia and hypotension indicative of intraabdominal hemorrhage or septic shock.
Fever: The fever of appendicitis, diverticulitis, and cholecystitis is typically low grade, whereas high fevers are seen in cases of cholangitis, urinary tract infections, pelvic inflammatory disease, or perforation of a viscus with frank peritonitis.
Inspection
Abdominal distention: Abdominal distention may suggest bowel obstruction or the presence of ascites.
Scaphoid abdomen: A scaphoid, tense abdomen is seen in cases of peritonitis.
Auscultation
Auscultation of the abdomen should be performed before palpation or percussion so as not to interfere with the interpretation of bowel sounds.
Absence of bowel sounds: Absence of bowel sounds is a sign of diffuse peritonitis.
Hyperactive bowel sounds: Intermittent hyperactive bowel sounds occurring concurrently with worsening of pain suggest a bowel obstruction. High-pitched hyperactive bowel sounds may also be seen in gastroenteritis.
Succussion splash: The presence of a succussion splash suggests gastric outlet obstruction.
Percussion
Tenderness on percussion: Percussion of the abdomen allows assessment of the presence of peritonitis. Pain produced by light tapping indicates inflammation of the parietal peritoneum. This pain may also be elicited by asking the patient to cough or by gently agitating the gurney upon which the patient is lying.
Tympany: A distended abdomen with tympany upon percussion suggests a bowel obstruction.
Palpation
Tightening (rigidity) of the abdominal wall musculature occurs as a reflexive response to peritoneal inflammation (voluntary guarding refers to tightness or rigidity of the abdomen that relaxes when the patient takes a deep breath, whereas involuntary guarding refers to rigidity of the abdominal wall musculature that does not relax in response to deep inspiration). Involuntary guarding indicates peritoneal inflammation.
Tenderness over McBurney’s point should be considered very strong evidence of appendicitis.
Cholecystitis and salpingitis are often well localized as well, and salpingitis may be confused with appendicitis.
Patients with an unimpressive abdominal examination and complaints of severe, worsening pain should be suspected of having mesenteric infarction.
Murphy’s sign refers to pain produced by deep inspiration during palpation of the right subcostal area and suggests acute cholecystitis.
Pain produced by lightly punching the costovertebral angle (”punch tenderness”) is often present in pyelonephritis.
Carnett’s test refers to the response of pain when the patient tenses the abdominal wall muscles by raising their head off the examination table. Worsening of pain during this maneuver suggests an abdominal wall source whereas improvement in the pain suggests a visceral origin.
The iliopsoas sign refers to pain produced by passive extension of the leg and suggests a psoas abscess.
The obturator sign refers to pain produced by rotation of the thigh in a flexed position.
A rectal examination can reveal focal tenderness from an intraabdominal abscess or appendicitis.
A pelvic examination is mandatory in female patients to look for evidence of salpingitis or adnexal masses.
The inguinal and femoral canals, umbilicus, and surgical scars should be evaluated for the presence of incarcerating hernias.
Once a cause is suspected the appropriate diagnostic procedure for the provisional diagnosis is selected.
Diagnosis
If the picture is obscure then the following important points and causes should be taken into account:
Ruptured ectopic pregnancy in females
Dissecting aortic aneurysm: Absence of tenderness and rigidity in the presence of continuous, diffuse pain in a patient likely to have vascular disease is quite characteristic of occlusion of the superior mesenteric artery. Abdominal pain with radiation to the sacral region, flank, or genitalia should always signal the possible presence of a rupturing abdominal aortic aneurysm. This pain may persist over a period of several days before rupture and collapse occur.
Peritoneal pain: Rigidity, rebound tenderness, fever and leucocytosis
Metabolic causes
Familial mediterranean fever
Diabetic ketoacidosis
Irritable bowel syndrome: Is the commonest cause of abdominal pain and should always be kept in mind.
If the cause of abdominal pain is still unclear, investigations that can be requested include:
Lab work
X-rays (supine, erect, lateral view)
Ultrasound
CAT scan
Laparoscopy
Operation vs. watchful waiting
Chronic abdominal pain
Chronic pain usually has persisted for 3 to 6 months and is affecting the patient’s activities of daily living. Often, the diagnosis can be made through history taking.
Chronic epigastric pain can be caused by peptic ulcer, chronic pancreatitis, GERD, dyspepsia, gall bladder disease.
Chronic lower abdominal pain can be caused by irritable bowel syndrome, inflammatory bowel disease, cancer. Right lower quadrant fullness and pain or perianal disease may indicate Crohn’s disease.
Less common causes include causes in the abdominal wall, fibromyalgia, hernia, referred pain, metabolic disorders (porphyria, chronic renal failure, and Addison’s disease) and psychological disorders.
The evaluation of chronic abdominal pain in a patient younger than 50 years old typically begins with ruling out the presence of alarm symptoms (weight loss, gastrointestinal bleeding, anemia, fever, or frequent nocturnal symptoms).
If no alarm symptoms are present and the patient has altered bowel habits then evaluation for irritable bowel syndrome is considered. This my include a CBC, TSH and electrolyte levels, and examination with flexible sigmoidoscopy.
Those with alarm symptoms or age above 50 years old may require a referral to a gastroenterologist.
{kind=link}
Related;
.
No comments:
Post a Comment